Adrenaline Surges in Severe ME… Dangers and Appropriate Action
Lack of Research, Common Report
Adrenaline surges are one of the most commonly shared experiences in ME and particularly severe ME groups. Despite this, I could not find any formal studies on adrenaline surges in ME. However, The Hummingbird Foundation does provide an excellent overview of adrenaline surges in ME which I recommend. Therefore the information in this post is based on anecdotal reports and case studies. However, I do aim to focus on only the most common and undebated areas of this discussion.
https://www.hfme.org/adrenalinesurgetips.htm
Please also be aware that adrenal insufficiency and adrenal dysfunction is a common causes of chronic fatigue, but that resources related to adrenal insufficiency do not apply to ME patients unless they have a comorbid diagnosis and are different from this discussion.
-------
What is an adrenaline surge?
Adrenaline is a hormone or chemical messenger that is released during the fight or flight reflex. In other words, it is a temporary burst of energy our body produces to get us out of a dangerous situation.
In people with ME, adrenaline surges can appear to be a magical blessing. This burst of energy often comes when we most need it (triggered by stress) and allows us to suddenly perform tasks that were previously impossible. Adrenaline surges in ME can last anywhere from an hour to months, with a few hours or days being the most common.
The problem is that adrenaline is temporary. So when an adrenaline rush wears off patients experience severe PEM. This is the danger of adrenaline. It allows us to override our bodies' natural protection against PEM: fatigue.
------
Adrenaline As Debt
A great metaphor given by ME patient Clytie is to think of adrenaline like debt.
If I asked you to go out and buy a Ferrari you would probably tell me you can't afford it.
But that's wrong. You could sell your house, open a bunch of credit cards, sell some drugs, rob a bank, and then go buy a Ferrari and you would have one.
Until the police and the debt collectors come knocking and you end up in prison or dead.
That's what using adrenaline to do things is like for people with ME. It might feel good or get us respect for a minute, but it's a terrible decision.
In the case of severe ME adrenaline surges are particularly dangerous. A severe crash for these patients can mean inability to swallow, difficulty breathing, low oxygen, and dysautonomia to the point of life-threatening blood pressure or heart rates.
------
So Why Do We Do It?
There are tons of reasons people with ME use adrenaline surges but some of the most common are:
Lack of Awareness & Gaslighting
Necessity
Adrenaline Surges*
*Yup! It's recursive!
I want to stress that while using adrenaline is often a mistake in the sense that patients would be better off if they did not do it, this doesn't mean patients are at fault for these mistakes. All are making their best judgement in an attempt to get better and a lack of awareness and accommodation makes using adrenaline common.
------
Lack of Awareness & Gaslighting
ME often has a sudden onset. When patients first become sick they expect to get better. Adrenaline surges make them feel how they expect to feel. They assume recovery, not false energy. This pattern of feeling better, doing more, and then crashing into PEM is often called the "push crash cycle*" and learning to identify it is a primary tennent of pacing. This is the easiest area to fix because once patients learn this pattern they will generally take steps to avoid it.
Medical gaslighting however can perpetuate this cycle. If patients are given CBT or GET that encourages the push half of the cycle, they will continue to utilize adrenaline surges in an attempt to meet the unrealistic standards placed upon them. Even once these programs are continued the mentality of "if I can do it I should try" persists.
*The push crash cycle is sometimes used to make patients feel responsible for their decline. This is BS. Our society makes this cycle the expected response to ME and patients are not at fault for falling into it.
------
Necessity
Unfortunately, many people with ME use adrenaline surges despite awareness of risk out of necessity. Patients know that they must pay a bill, buy groceries, or attend a medical visit to survive and that without adrenaline they would simply be unable to complete this task. They make the difficult decision to sacrifice long-term health in order to survive.
Whitney Dafoe writes in "Extremely Severe ME; A Personal Account" that adrenaline surges are what (most of the time) allow him to get to a toilet to poop. For those living without a caregiver, the choice may be to use the adrenaline or to sit in your own filth.
This is ultimately a problem that only a real social safety net and care for ME patients will resolve.
-------
Recursive Adrenaline Surges
Adrenaline itself causes us to misuse adrenaline surges.
Adrenaline makes us more impulsive leading to unwise choices about activity.
It also stops us from sleeping causing us to do activity. In turn sleep deprivation causes adrenaline release which can prolong this cycle.
Finally, people who misuse adrenaline surges regularly are more likely to become severe or very severe. This means they may then be dependent on using adrenaline for basic necessities. The more severe you are the greater the temptation to use adrenaline due to the severe mental strain of solitary confinement, sensory deprivation, and extreme boredom.
-------
Harm Reduction
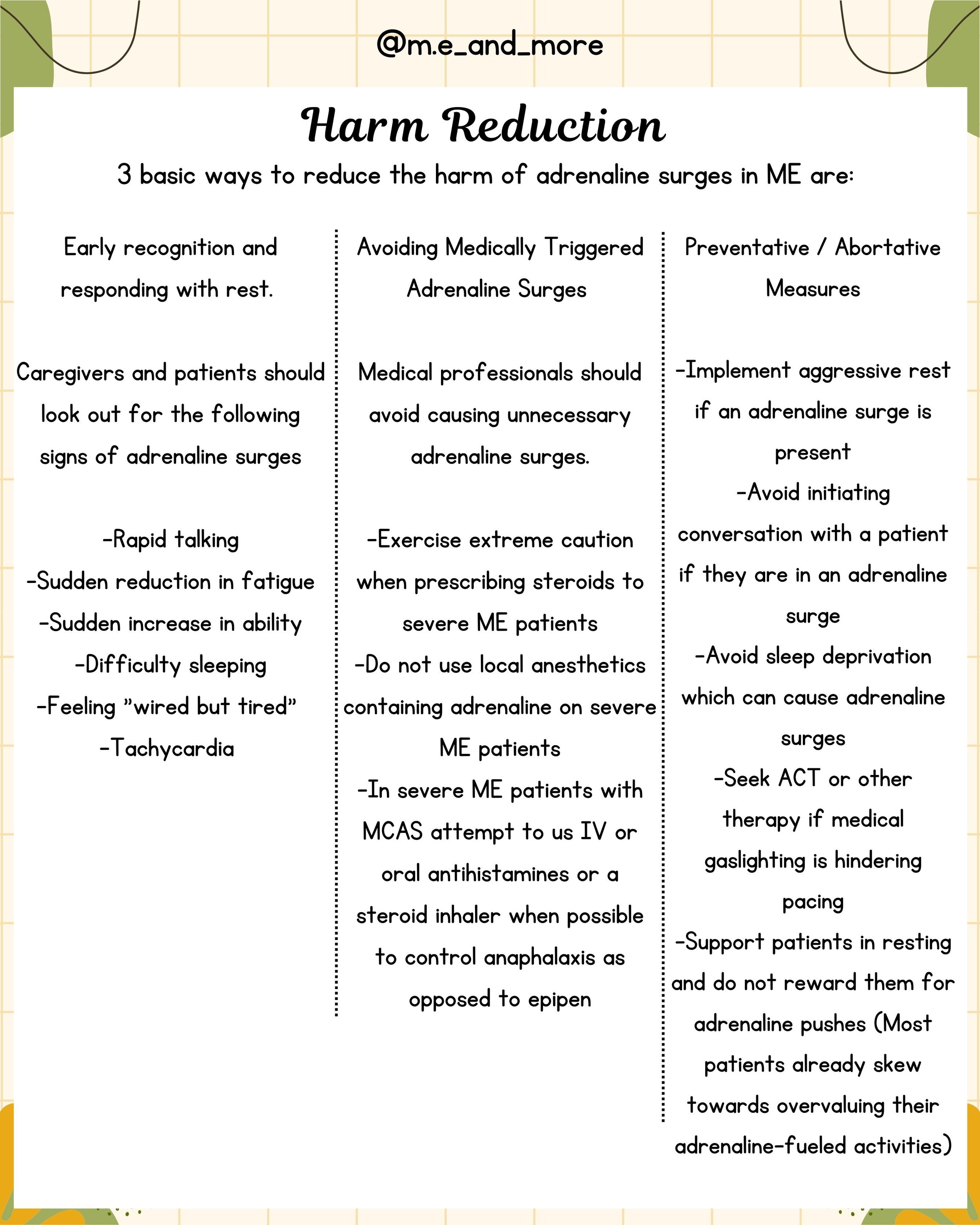
3 basic ways to reduce the harm of adrenaline surges in ME are:
Early recognition and responding with rest.
Caregivers and patients should look out for the following signs of adrenaline surges
-Rapid talking
-Sudden reduction in fatigue
-Sudden increase in ability
-Difficulty sleeping
-Feeling "wired but tired"
-Tachycardia
Avoiding Medically Triggered Adrenaline Surges
Medical professionals should avoid causing unnecessary adrenaline surges.
-Exercise extreme caution when prescribing steroids to severe ME patients
-Do not use local anesthetics containing adrenaline on severe ME patients
-In severe ME patients with MCAS attempt to use IV or oral antihistamines or a steroid inhaler when possible to control anaphylaxis as opposed to epipen
Preventative / Abortative Measures
-Implement aggressive rest if an adrenaline surge is present
-Avoid initiating conversation with a patient if they are in an adrenaline surge
-Avoid sleep deprivation which can cause adrenaline surges
-Seek ACT or other therapy if medical gaslighting is hindering pacing
-Support patients in resting and do not reward them for adrenaline pushes (Most patients already skew towards overvaluing their adrenaline-fueled activities)
------
Need For Change
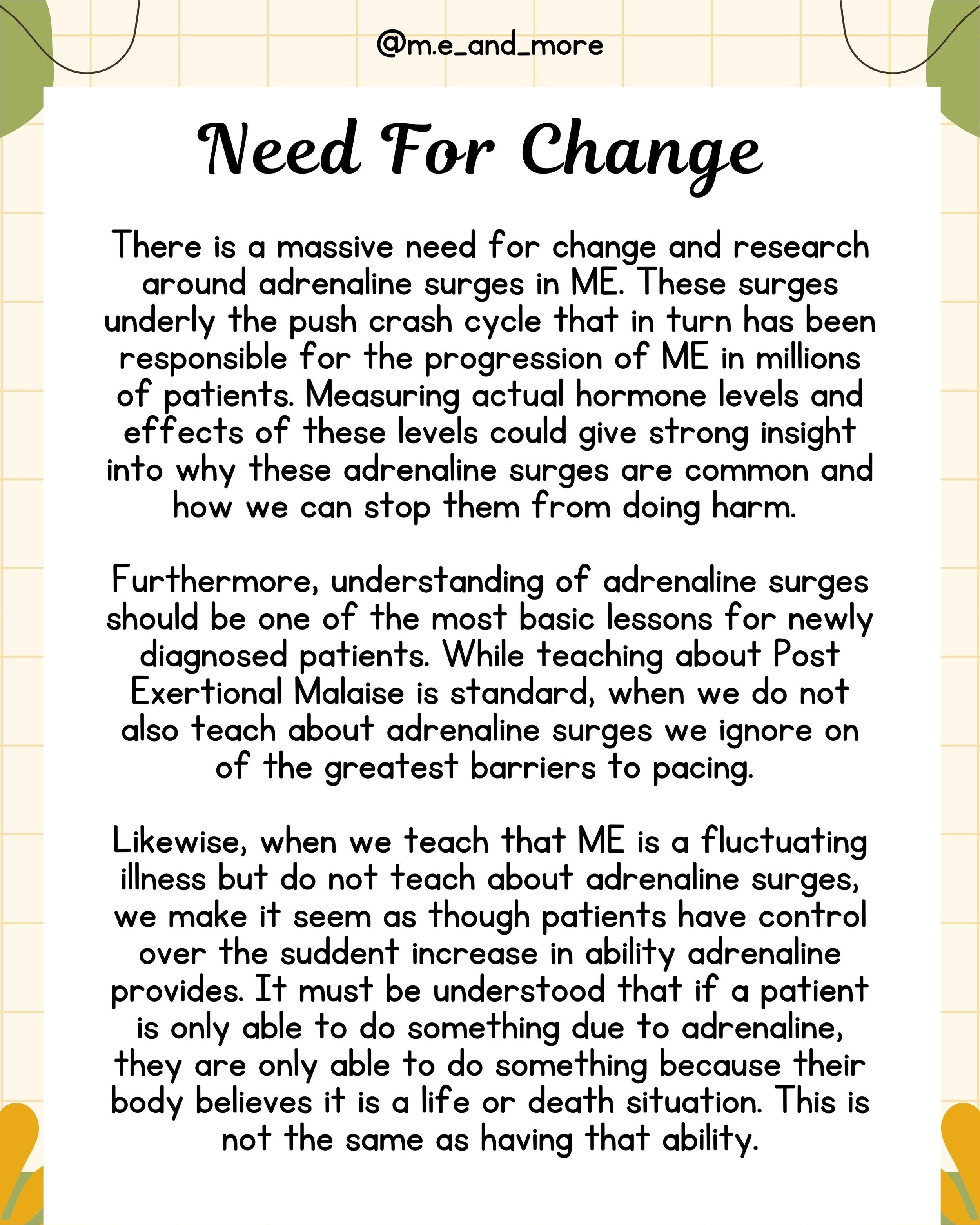
There is a massive need for change and research around adrenaline surges in ME. These surges underly the push crash cycle that in turn has been responsible for the progression of ME in millions of patients. Measuring actual hormone levels and effects of these levels could give strong insight into why these adrenaline surges are common and how we can stop them from doing harm.
Furthermore, understanding of adrenaline surges should be one of the most basic lessons for newly diagnosed patients. While teaching about Post Exertional Malaise is standard, when we do not also teach about adrenaline surges we ignore on of the greatest barriers to pacing.
Likewise, when we teach that ME is a fluctuating illness but do not teach about adrenaline surges, we make it seem as though patients have control over the sudden increase in ability adrenaline provides. It must be understood that if a patient is only able to do something due to adrenaline, they are only able to do something because their body believes it is a life-or-death situation. This is not the same as having that ability.
------
Adrenaline and MECFS are a dangerous combination.
wired but tired is a common phrase in Myalgic Encephalomyelitis groups that refers to when we are exhausted but unable to sleep. This feeling is often the reason patients, even those who understand the dangers, fail to pace.
Despite the fact that this experience is very commonly reported in ME and severe ME patients, there is no formal research into adrenaline surges in ME. This needs to change. Adrenaline surges are likely responsible for much of the decline that ME patients experience. They often underly the push crash cycle and can make pacing difficult or impossible.
Natural adrenaline surges are a problem in ME. But adrenaline surges can also be induced through the use of steroids like prednisone, epinephrine injections (epipen), or adrenaline in local anesthetics. Awareness of the dangers these medications pose in ME especially severe and very Severe ME is essential to minimizing damage by increasing awareness, encouraging aggressive rest, and prescribing appropriate sedating drugs to ensure adequate sleep.
Many patients report that adrenaline surges can also be triggered by overtiredness. Therefore it is important for anyone with ME to be mindful of staying up for too many hours continuously. This can be a recursive issue as adrenaline makes it difficult to sleep and drugs may be needed to break the cycle.
It's important to remember that adrenaline surges aren't your fault and cloud your judgement. They often lead to mistakes and failing to Stop Rest Pace but this should not be blamed on the patient. Instead, appropriate psychological and pharmaceutical tools should be given to patients to allow them to safely get through the surge.
Meditation, vagus nerve stimulation, and other mindfulness activities can be helpful in lowering our fight or flight reflex and controlling adrenaline surges. I believe controlling adrenaline is the primary reason that some people see success with psychologically based programs despite the fact ME cannot be cured psychologically.